SUBMIT YOUR MANUSCRIPT
Affiliations
ABSTRACT
Anatomical variations of biliary and vascular structures may affect the safe performance of cholecystectomy during a surgery. A 58-year female patient was admitted to the emergency department with a complaint of right upper quadrant pain and was diagnosed with cholelithiasis and acute cholangitis, and hence was admitted. Cholecystectomy was planned under elective conditions and surgery preparations were completed. The operation was started in accordance with the American cholecystectomy technique. During exploration, it was observed that the cystic artery was originating from Calot's triangle anastomoses with a separate cystic artery originating from the falciform ligament and entering from the corpus of the gallbladder. The cystic artery originating from the falciform ligament was clipped with an endoclip and then cut. Although rare, anatomical variations should be considered individually for each cholecystectomy case because these can result in complications.
Key Words: Cystic artery, Laparoscopic cholecystectomy, Anatomical variations.
INTRODUCTION
Laparoscopic cholecystectomy is the standard treatment for cholelithiasis.1 Anatomical variations in the biliary and vascular structures may affect the safe performance of cholecystectomies. Variations in cystic artery anatomy are common.2 Therefore, injuries may occur during the surgery. The incidence of conversion from laparoscopic to open surgery due to vascular injuries has been reported to be 0-1.9%.3 It has also been reported that the mortality rate due to bleeding after injury is 0.02%.3 To prevent injuries, the critical view of safety (CVS) procedures and principles, as well as the experience and knowledge of surgeons, have been adopted.4
We present a case of a 58-year female patient admitted to the emergency department with a complaint of right upper quadrant pain and diagnosed with cholelithiasis and acute cholangitis. During laparoscopic cholecystectomy, an aberrant cystic artery was found and was managed successfully.
CASE REPORT
A 58-year female patient was admitted to the emergency department complaining of right upper quadrant pain. She was diagnosed with cholelithiasis and acute cholangitis, and was admitted to the clinic. The medical treatment was initiated, and magnetic resonance cholangiopancreatography (MRCP) was performed. Because millimetric-sized calculi were observed on MRCP causing obstruction in the distal common bile duct, stone extraction was performed via endoscopic retrograde cholangiopancreatography (ERCP), and a biliary stent was inserted. The patient was discharged after her clinical condition improved and treatment was completed.
Approximately 6 weeks later, the patient was called for a check-up, and the biliary stent was removed via ERCP. In the control MRCP, the common bile duct and intra- and extrahepatic bile ducts were open. Calculi, the largest of which was 22 mm in diameter, were observed in the gallbladder. Cholecystectomy was planned under elective conditions and the surgical preparations were completed.
A surgery was performed in accordance with the American cholecystectomy technique.5 After the gallbladder was suspended from the fundus, dissection was initiated using a monopolar cautery, and the cystic duct and cystic artery were exposed. During the exploration, it was observed that the cystic artery originating from Calot's triangle merged with a separate cystic artery originating from the falciform ligament and entering from the corpus of the gallbladder. The cystic artery and duct in Calot’s triangle were dissected, clipped, and transected (Figure 1). The cystic artery originating from the falciform ligament was clipped using an endoclip and transected (Figure 2). It was resected retrogradely from the gallbladder bed using monopolar cautery, and the specimen was removed from the abdomen using an endobag. After haemostasis, the trocar sites were closed in accordance with the anatomy, and the operation was completed.
Since the patient’s postoperative abdominal examination and laboratory values were normal, she was discharged to the outpatient clinic with recommendations.
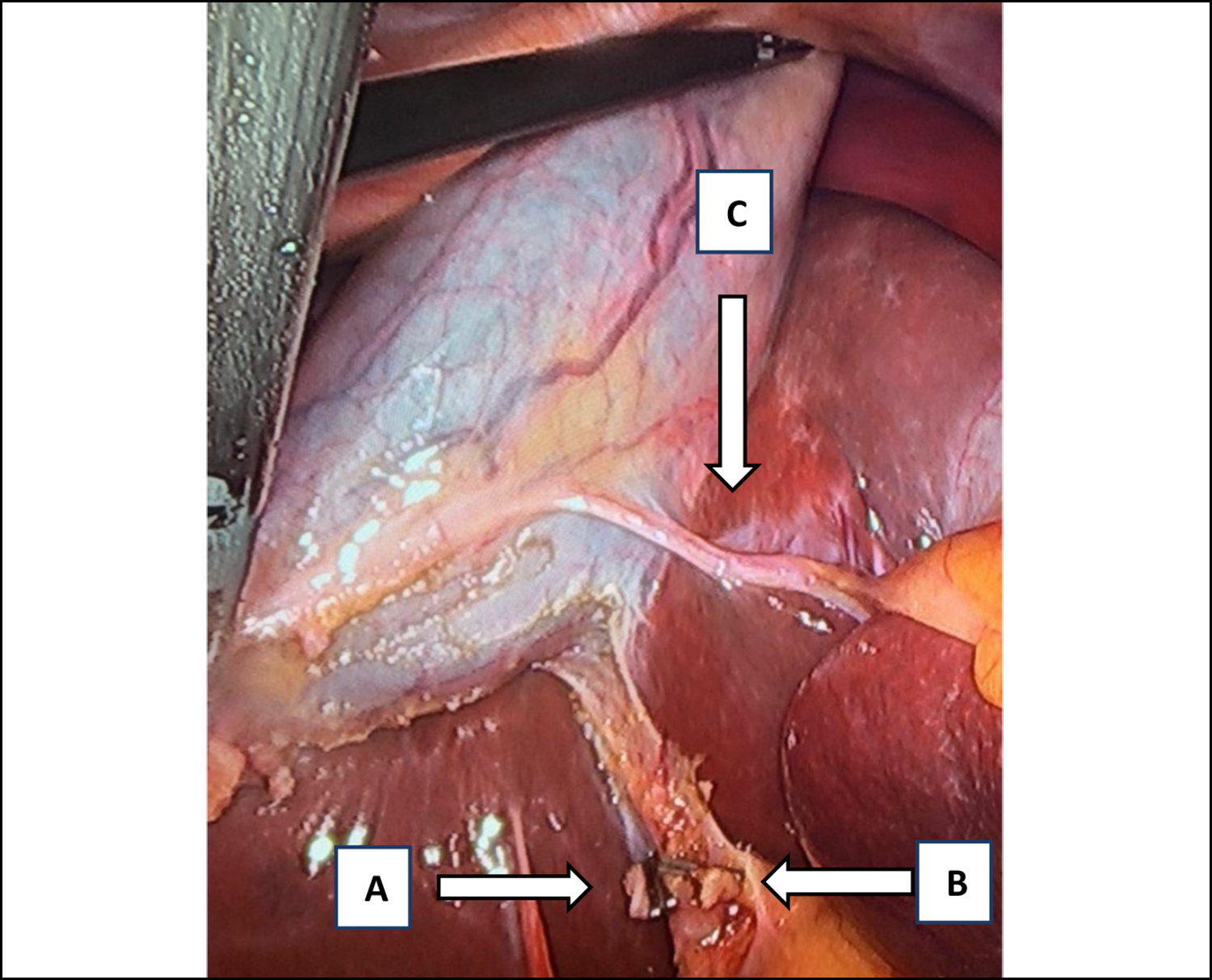 Figure 1: Intraoperative findings during the surgery; (A) Cystic duct (B) Cystic artery (C) The second cystic artery.
Figure 1: Intraoperative findings during the surgery; (A) Cystic duct (B) Cystic artery (C) The second cystic artery.
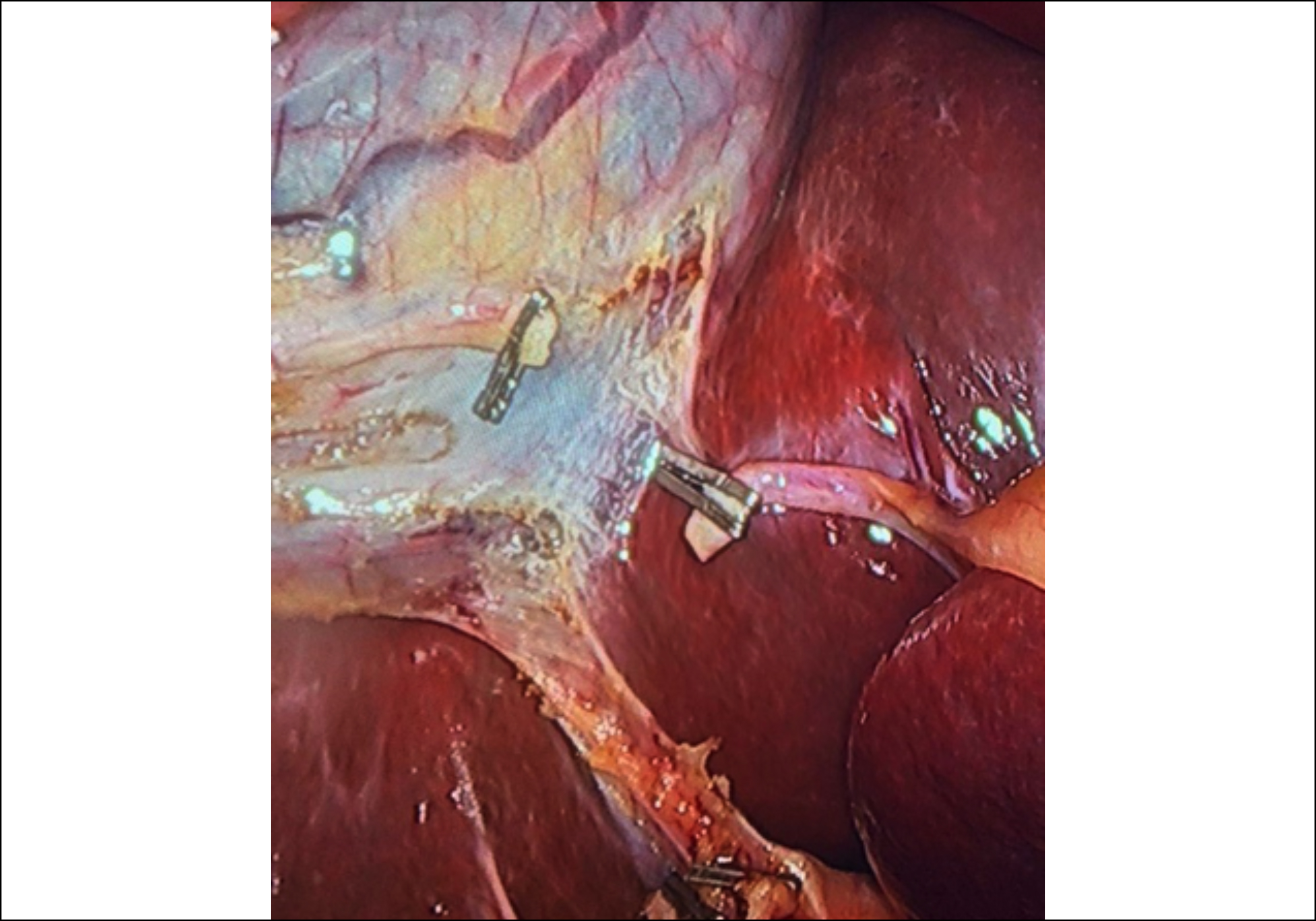 Figure 2: Intraoperative findings after ligation during the surgery.
Figure 2: Intraoperative findings after ligation during the surgery.
DISCUSSION
The cystic artery mostly originates from the right hepatic artery (79.02%). Although there are rare cases in which a cystic artery is not observed (0.34%), double cystic arteries can also be observed (8.9%). The cystic artery may originate from the left hepatic artery (2.07%), gastroduodenal artery (1.94%), or from the proximal part of the right hepatic artery, where it either passes in front of the common bile duct (5.4%) or passes under the cystic duct (4.9%).6 These variations observed in the hepatocystic triangle can lead to the right hepatic artery being incorrectly identified as the cystic artery during dissection in Calot's triangle and increase the risk of injury during the surgery; however, in the previous study on the variations of the cystic artery, the cystic artery originating from the falciform ligament was not mentioned.6
To prevent complications that may occur due to anatomical variations found during open or laparoscopic cholecystectomies, it is necessary to first know the anatomy of this region. This region, called Calot's triangle, was first described in 1891.7 The CVS principles defined in this triangle are determined in three stages to prevent injuries. Dissection in Calot’s triangle is defined as the separation of the lower part of the gallbladder from the bladder bed and revealing the cystic duct and cystic artery, which are tubular structures.8
Although injuries to the common bile duct and vascular structures can often be prevented using safe cholecystectomy principles, it has been reported that there is a risk of 0.3-0.5% of common bile duct injuries.9 However, as the studies on the incidence of vascular injuries are insufficient, there is no specific rate in the literature on vascular injuries.4
Kim et al. reported an example of a cystic artery originating from the falciform ligament in a case report. In their case, after cystic artery ligation in Calot's triangle during CVS, a second cystic artery originating from the falciform ligament was observed, which was later defined as the artery of the hepatic artery segment 4.10 In the present case, the cystic duct and cystic artery structures were clearly defined within the safe cholecystectomy margins, which were identified during dissection in the Calot’s triangle. It was determined that the cystic artery merged with another cystic artery, coursing through the falciform ligament to the corpus of the gallbladder.
To prevent the surgical injuries, dissection should be performed carefully by the surgeon, and the steps followed for CVS should be observed.4 Advanced vascular imaging techniques can be used to detect vascular anomalies; however, additional imaging methods are not used because these anomalies are generally not predicted in the preoperative evaluation owing to their low incidence,. No additional imaging methods were used to investigate anomalies in our patient before the surgery.
Although rare, anatomical variations should be considered individually for each cholecystectomy case because they can cause complications. CVS should be followed to prevent injury and should be the first choice for all classical or laparoscopic gallbladder surgeries.
PATIENTS’ CONSENT:
Informed consent was obtained from the patient.
COMPETING INTEREST:
The authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
SY: Designed the work, analysed the data.
CO, HB: Collected the data.
OS: Analysed the data.
All authors approved the final version of the manuscript to be published.
REFERENCES